The government’s efforts to coerce healthcare providers to meaningfully use electronic health records is in full swing. Stage 1 of Meaningful Use (MU) focuses on electronic collection of data. Financial incentives have been provided for early adopters. Starting in 2015 penalties will be imposed for CMS related services, starting at 1% in 2015 and increasing by 1% each year up to 5%. Stage 2 addresses increasing quality, health information exchange, and patient engagement. Stage 3 targeted now for 2017 focuses on improving patient outcomes and population health.
What does Meaningful Use mean for DXA providers?
To participate in Meaningful Use a hospital or provider must comply with mandatory (Core) and elective (Menu) measures. Many measures define a degree of compliance. For example, 30% of all orders must be made via computerized provider order entry (CPOE). There is some flexibility in how compliance may be calculated. One key aspect for DXA providers is the classification of a patient encounter as “seen by” or an “office visit”. Patients “seen by” a physician may be excluded from measurements.
DXA providers may be considered specialists and thus be excluded from many aspects of meaningful use (see the Meaningful Use For Specialists Tip Sheet). If each patient receives a consult, then each visit would likely be counted under meaningful use (an an “office visit”). If a provider simply scans patients and returns a report to a referring physician, these could be categorized as “outpatient” (or “seen by”) encounters and be excluded.
We have seen flexibility in how MU is calculated and, in particular, which patients are counted. In one case, a radiologist performed thousands of readings in a year with only a handful of consults. In this case, the radiologist claimed exclusion because so few office visits were performed. We have also seen cases where an organization decided to include readings.
DXA providers must ask themselves if they want to comply with the letter of the law or truly buy into the spirit of meaningful use. Of course there are other factors to consider such as one’s ability (financial, technical, logistical) to comply.
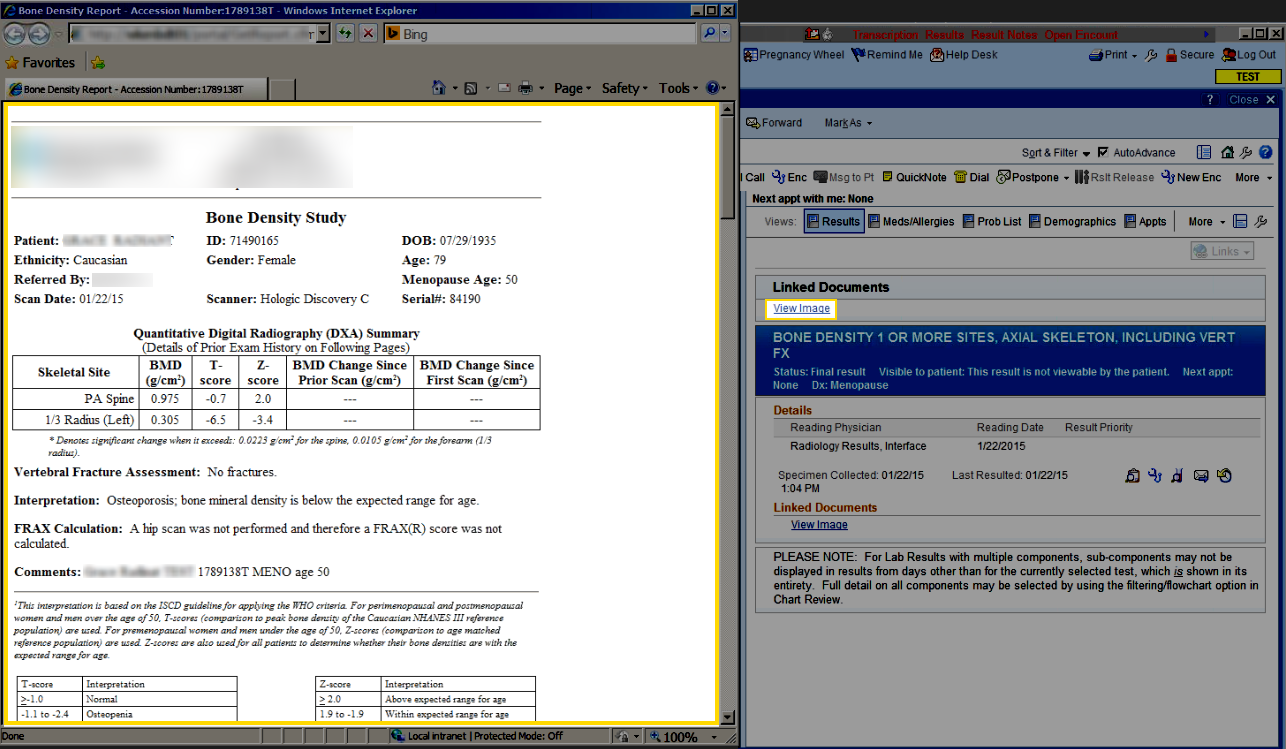
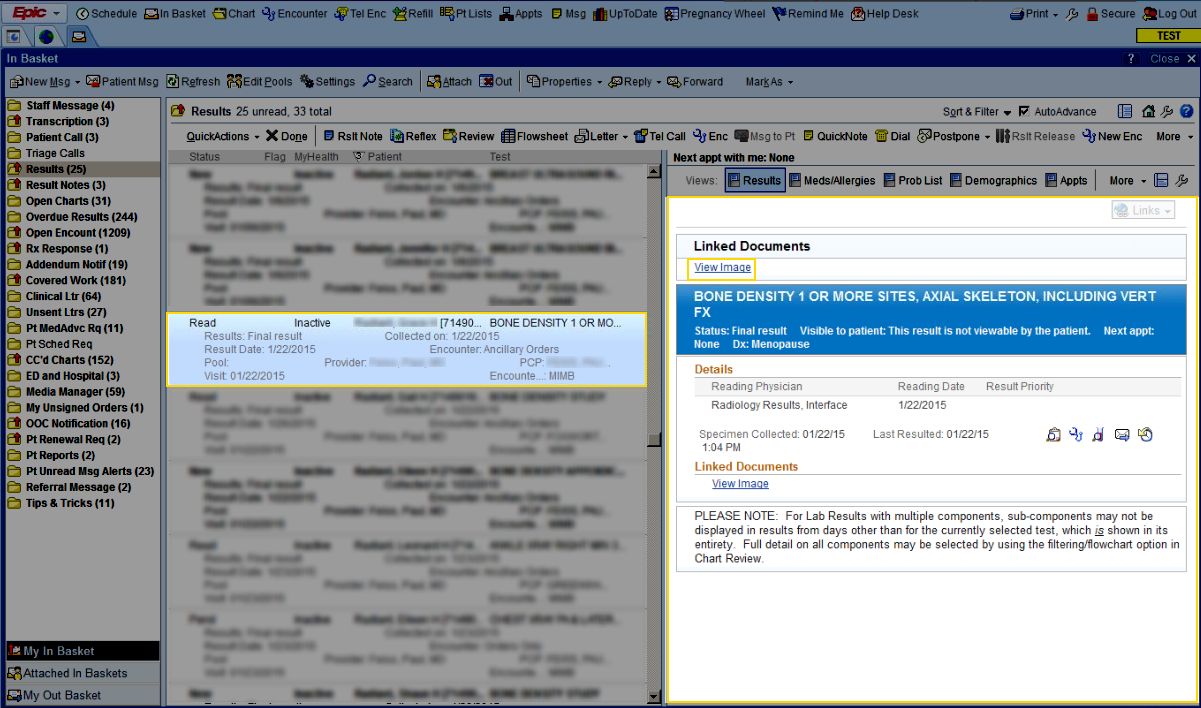
It may be difficult to avoid meaningful use, even as a specialist. Under Stage 1, 10% of all tests results must be provided to patients and this increases to 50% under Stage 2. DXA providers may be required to supply test results electronically as part of their hospital’s MU compliance. At the moment it is unclear as to whether images must be provided.
Another MU aspect which may be difficult to avoid is the collection of relevant patient demographics and history. For example, under Stage 1 patients’ ethnicity, height and weight must be collected as well as their smoking status. Many specialists may claim exclusion because these items are not relevant for their services. However, these items are necessary for DXA.
It may be relatively easy for some DXA providers to comply with MU. If your organization provides an EHR, you may be able to piggyback on them.
MU may also provide benefits for DXA. For example, a DXA operator doesn’t have to perform data collection if the data was already entered in the EHR (by another department for instance). There may be future benefits when the EHR can transfer appropriate data to the DXA machine – saving time by eliminating the technologist’s need to perform data re-entry. This is a perfect example of the spirit of meaningful use in action.
In this short article, we only touched the tip of the iceberg in terms of meaningful use for DXA. We hope to address related issues in future postings.
Helpful Links:
Stage 1 Core and Menu Measures
State 2 Core and Menu Measures