Introduction
Not much has changed in the dozen years since we wrote about DXA and PACs. Dictation is still a widely used tool, along side PACS, in reading bone density scans.
There are better ways to read DXA scans that minimize errors and produce better reports.
We have observed three problems with dictation that can easily be solved with a modern solution, such as BoneStation.
Errors capturing DXA data
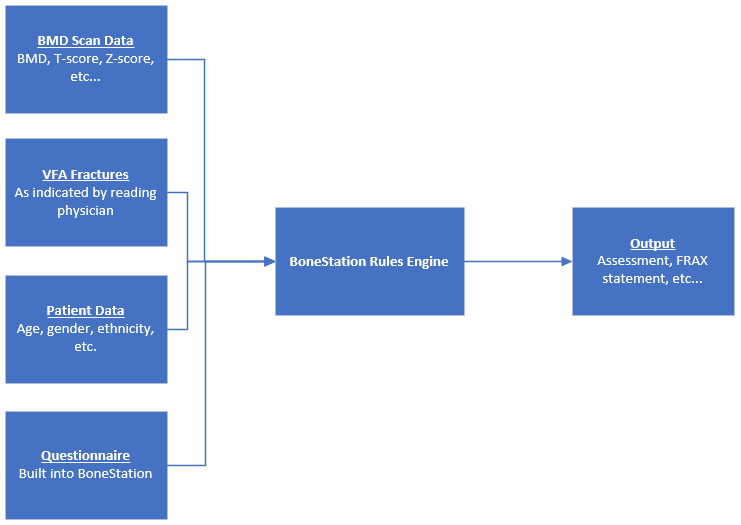
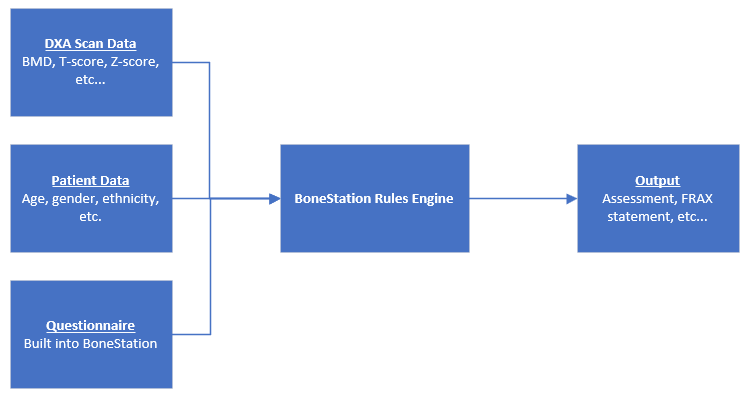
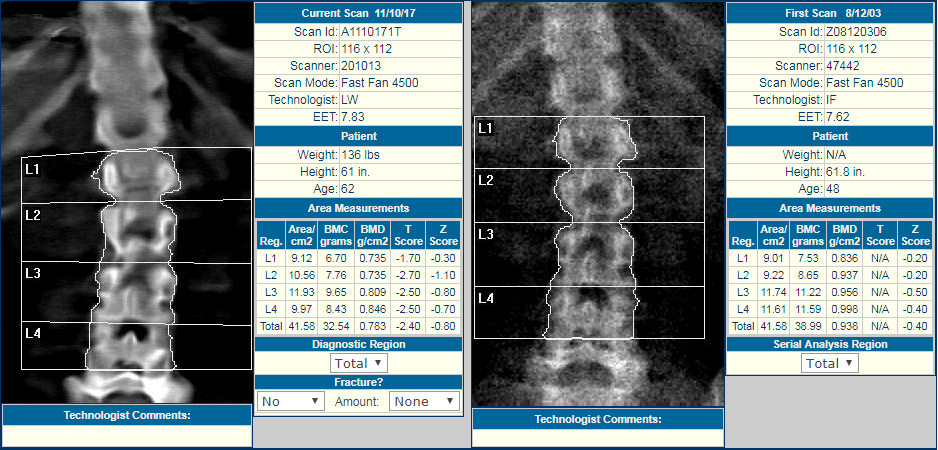
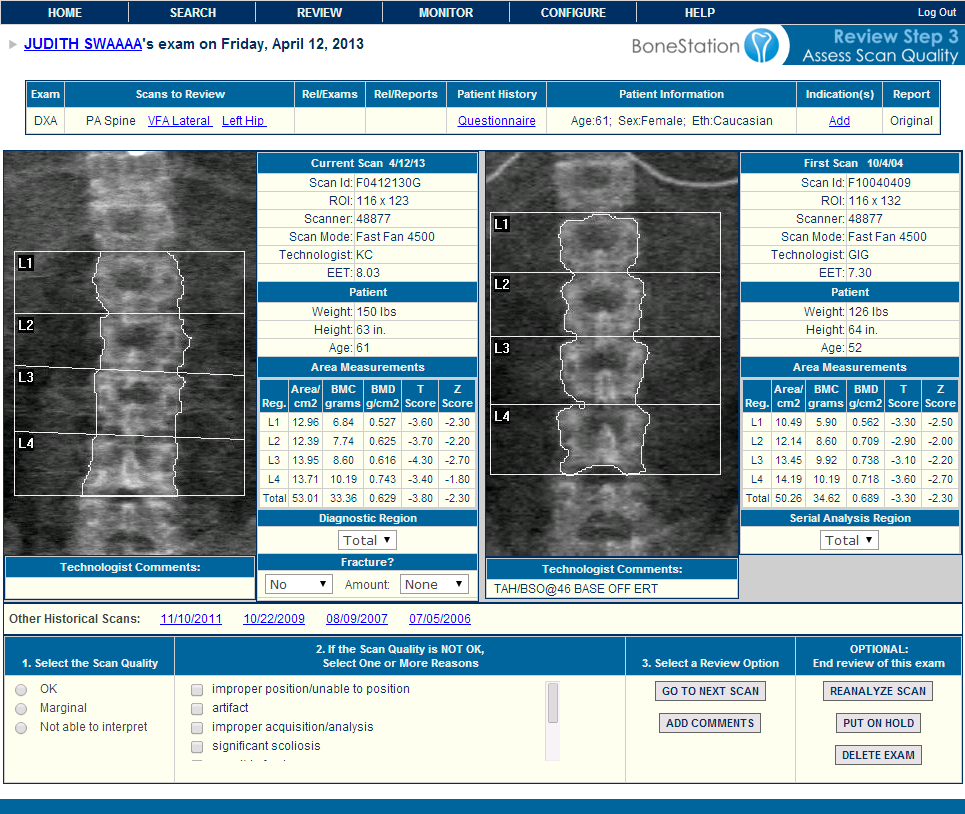
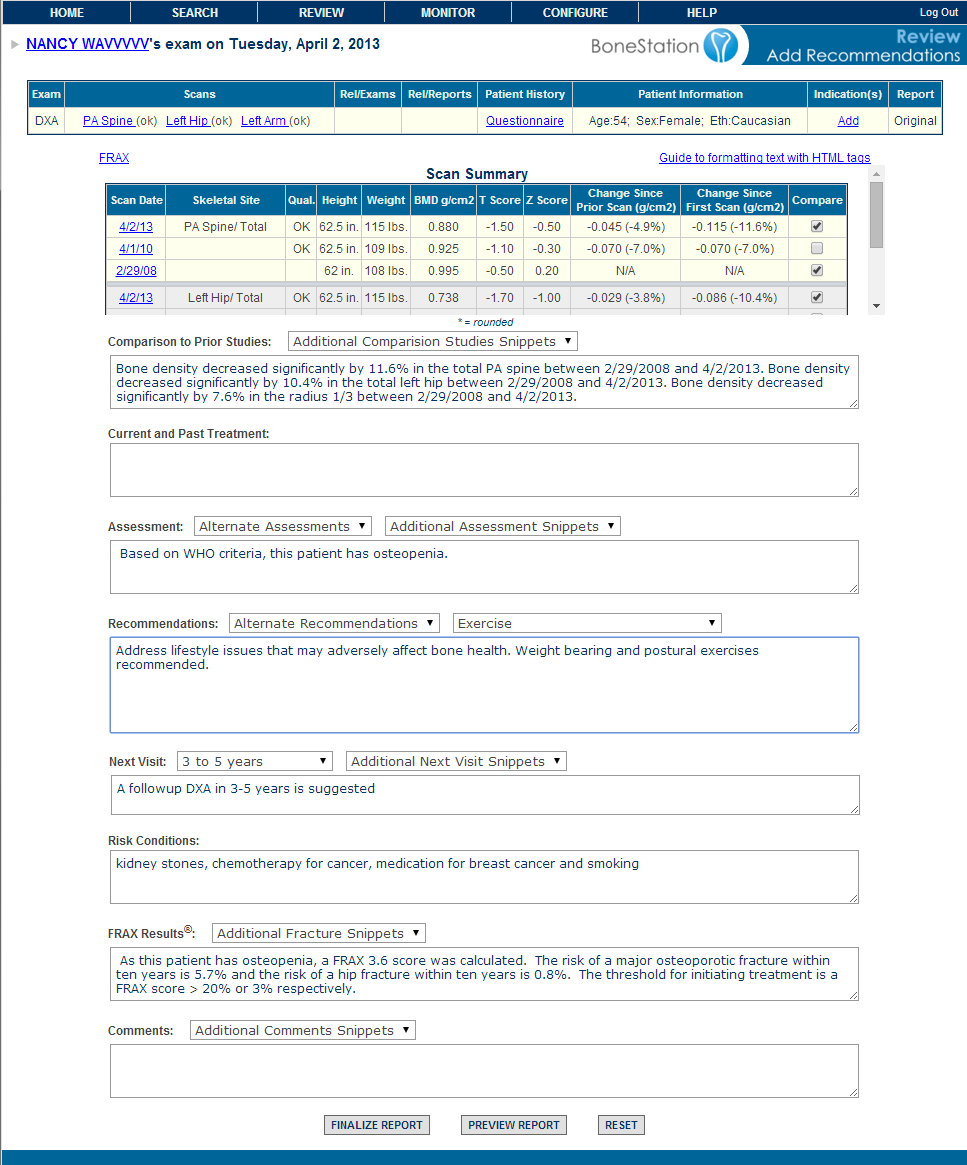
A DXA body density scan produces quantitative data, including clinically BMD, T-score, and Z-score. DXA readers will typically dictate these values to a report along with an interpretation.
The dictation process is a source of error. Research has found speech recognition software error rates of at least 7%.
Using modern tools, such as BoneStation, there is no need to dictate this information. BMD data can be captured automatically from the DICOM transmission of the scan. We talk about this in this blog post.
Tedious To Dictate Elements of a Good DXA Report
There are many components to a high quality bone density report, beyond the BMD data mentioned above. The International Society of Clinical Densitometry (ISCD) defines elements of a bone density report in its recommendations.
It is tedious for many readers of BMD scans to dictate all the elements of a high quality report. Often times this information is omitted. Items such as DXA machine make and model, FRAX risk factors, change in BMD and other clinically relevant information will be lacking from reports.
Time Consuming to Perform Calculations
It can be time consuming for a DXA reader to calculate useful BMD related values, such as change in BMD with prior scan, change in BMD with baseline, and least significant change (LSC).
Automated reporting software, such as BoneStation, can easily produce reports with change in BMD and LSC. In addition, BoneStation can automatically fill in other relevant data, such as DXA machine make and model, FRAX score, FRAX, risk factors, etc.
See our video on ISCD Report Compliance and BoneStation produced reports
Conclusion
Dictation is a widely used method to produce bone density reports today. It is fraught with problems, many of which also apply to transcription and templates. More modern methods exist, that can reduce errors while simultaneously improving quality and efficiency.